
Templates
Article.doc
Correspondance.doc
OpenEvaluation.doc
Consent form.doc
Licence CC-BY-SA.doc
Harlequin syndrome is a rare facial dysautonomic disorder first described in 1988 by Lance. The syndrome is characterized by erythematous dyschromia with hemifacial hyperhidrosis. Dyschromia and hyperhidrosis are well-defined at the midline and are also associated with contralateral anhidrosis. The condition results from unilateral disruption of sympathetic fibers at the level of vertebrae T2-T3. In most cases, the condition is idiopathic. However, several cases secondary to underlying cervical and upper thoracic pathologies, to cervico-thoracic surgical or anesthetic interventions, or to systemic diseases have been reported in the literature. Although it is a benign syndrome that often resolves spontaneously, its sudden, dramatic, and colorful onset can cause significant distress and anxiety for the patient and their family. A proper understanding of this syndrome enables clinicians to identify the condition and guide appropriate management.
Objective: The aim of this study is to evaluate whether the simultaneous removal of mandibular third molars during sagittal split osteotomy (SSO) influences the incidence and severity of postoperative neurosensory disturbances of the inferior alveolar nerve (IAN).
Material and methods: In this prospective cohort study, 172 SSO procedures were analyzed at the Department of Oral and Maxillofacial Surgery, AZ Vitaz Hospital, Belgium. Patients were divided into two groups: those with no third molars present (Group I, n = 117) and those undergoing simultaneous third molar removal during SSO (Group II, n = 55). Neurosensory function was evaluated at 1 day, 1 week, 3 weeks and 6 weeks postoperatively using objective (Medical Research Counsel (MRC) scale, two-point discrimination, static light touch, sharp/blunt discrimination) and subjective measures. Logistic regression and ANCOVA were used to assess associations between third molar status and neurosensory outcomes.
Results: In both groups, high sensory recovery rates were achieved six weeks after surgery: 91% and 95%, respectively. There were no statistically significant differences between the groups in terms of the duration required to reach functional sensory recovery (p = .650), final MRC score distribution (p = .702), two-point discrimination scores, or static light touch or sharp/blunt discrimination. Entrapment of the IAN occurred more frequently in patients with third molars (69.1% vs. 53.8%), but this difference was not statistically significant (p = 0.058). Entrapment and patient age were significant predictors of neurosensory complaints. No adverse outcomes occurred in either group.
Conclusions: Simultaneously removing mandibular third molars during SSO does not significantly impact postoperative neurosensory outcomes. Age and inferior alveolar nerve (IAN) entrapment are more critical risk factors for altered sensation. These findings support the safety of removing third molars at the same time as orthognathic surgery.
Foreign bodies in the oral cavity of infants are uncommon and often present with no specific symptoms, leading to frequent misdiagnosis. The anterior hard palate is an unusual site for foreign body impaction, but it can retain small objects due to its anatomical features. In this case, a nine-month-old boy was referred to as a suspicious palatal lesion, which was ultimately identified as a soft silicone foreign body. Early recognition and safe removal prevented further complications. This case highlights the importance of including foreign bodies in the differential diagnosis of palatal lesions, and the need for awareness across different disciplines and parental education.

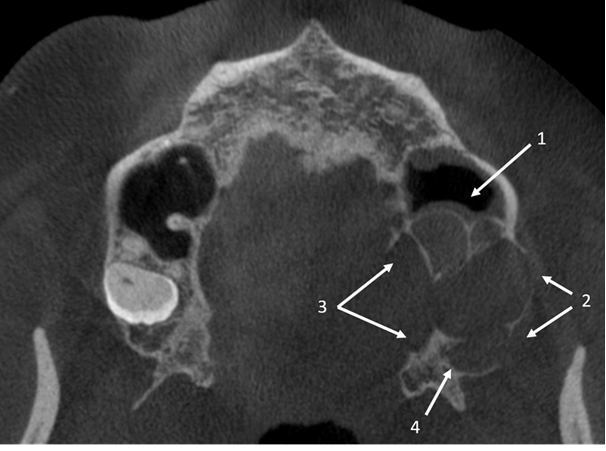
Les troisièmes molaires inférieures incluses et ectopiques, situées au niveau de l’incisure sigmoïdienne, sont très rares en pratique clinique. Leur étiologie demeure incertaine même si on soupçonne des perturbations du processus d'éruption dentaire ou des conséquences de traumatismes. La majorité des cas décrits dans la littérature présente divers symptômes et nécessite une prise en charge chirurgicale. L’objectif de ce travail est de réaliser une revue de la littérature sur les troisièmes molaires inférieures incluses et ectopiques dans la région de l’incisure sigmoïdienne, de présenter un nouveau cas clinique illustré par tomographie à faisceau conique (CBCT), et d’établir des stratégies de prise en charge possibles, en explorant les indications pour une intervention chirurgicale selon la littérature disponible.

L'ostéome est une tumeur ostéoblastique bénigne. Il se développe de préférence dans la région crâniofaciale, mais reste une tumeur rare. Il est souvent asymptomatique et découvert par hasard. Il peut se présenter sous la forme d'un gonflement osseux localisé, causant des préoccupations esthétiques et fonctionnelles pour les patients. Il est essentiel de comprendre les caractéristiques cliniques et radiologiques ainsi que le traitement afin d'assurer une prise en charge appropriée et efficace. Il existe des différences claires qui permettent de distinguer l'ostéome de l'ostéome ostéoïde mandibulaire. Bien que le pronostic de l'ostéome mandibulaire soit généralement favorable, il est essentiel de connaître cette affection pour pouvoir la diagnostiquer et la prendre en charge à temps, notamment afin de la différencier des lésions plus agressives de la mâchoire.
Odontomas are benign odontogenic tumors resulting from developmental defects in dental tissues. They are categorized into two types: complex odontomas, composed of disorganized dental tissue masses, and compound odontomas, characterized by multiple, tooth-like structures. This case report describes an unusual instance of a compound odontoma in the anterior mandible of a 7-year-old male, detected incidentally during a routine dental check-up. Radiographic imaging, including panoramic X-ray and CBCT, revealed a hyperdense, tooth-like mass in the anterior left mandible. The lesion was surgically removed under general anesthesia, resulting in the extraction of 56 denticles. Postoperative recovery was uneventful, and no recurrence was observed. Although odontomas are generally asymptomatic, early detection and timely surgical intervention are crucial to prevent complications such as impacted teeth. The prognosis is typically favorable, with a low risk of recurrence.
The cases of a ballistic projectile entering the pterygopalatine fossa are rare (8 reported cases), and the procedure of removing a foreign body from this anatomical space requires an operator’s experience and appropriate attention. We report the second case of a bullet from a non-powder weapon in the pterygopalatine fossa described in the English literature and the first removed by open trans-sinusal surgery. A 53-year-old male patient was shot and referred from another hospital for removal of a bullet from the pterygopalatine fossa. The patient had a craniofacial CT scan and was in good general condition. The foreign body was trans-sinusally non-endoscopically removed. The experience, knowledge and manual dexterity of the operator allowed avoiding iatrogenic complications such as intraoperative bleeding and nerve injury. The basis for a successful operation was good diagnostic, including radiological diagnostic consisting of performing a cranio-facial CT scan.
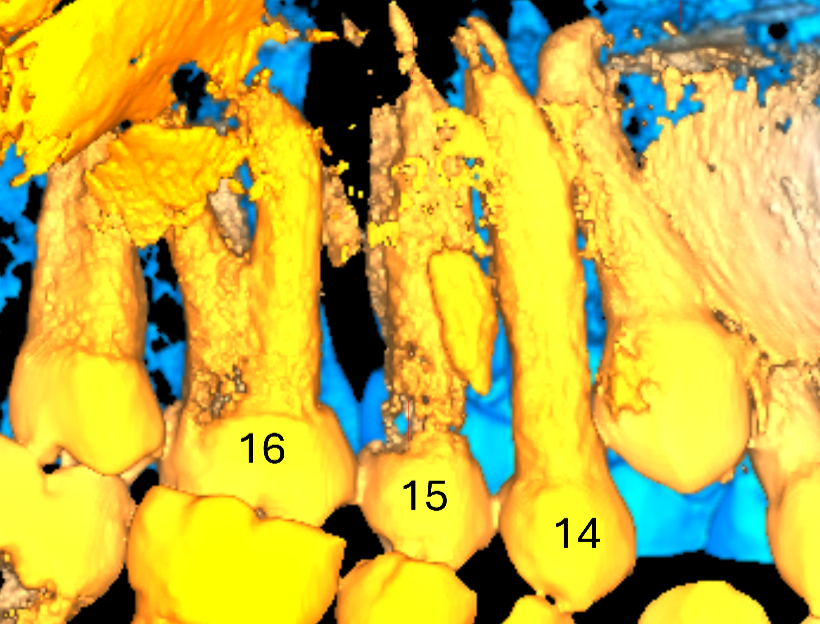
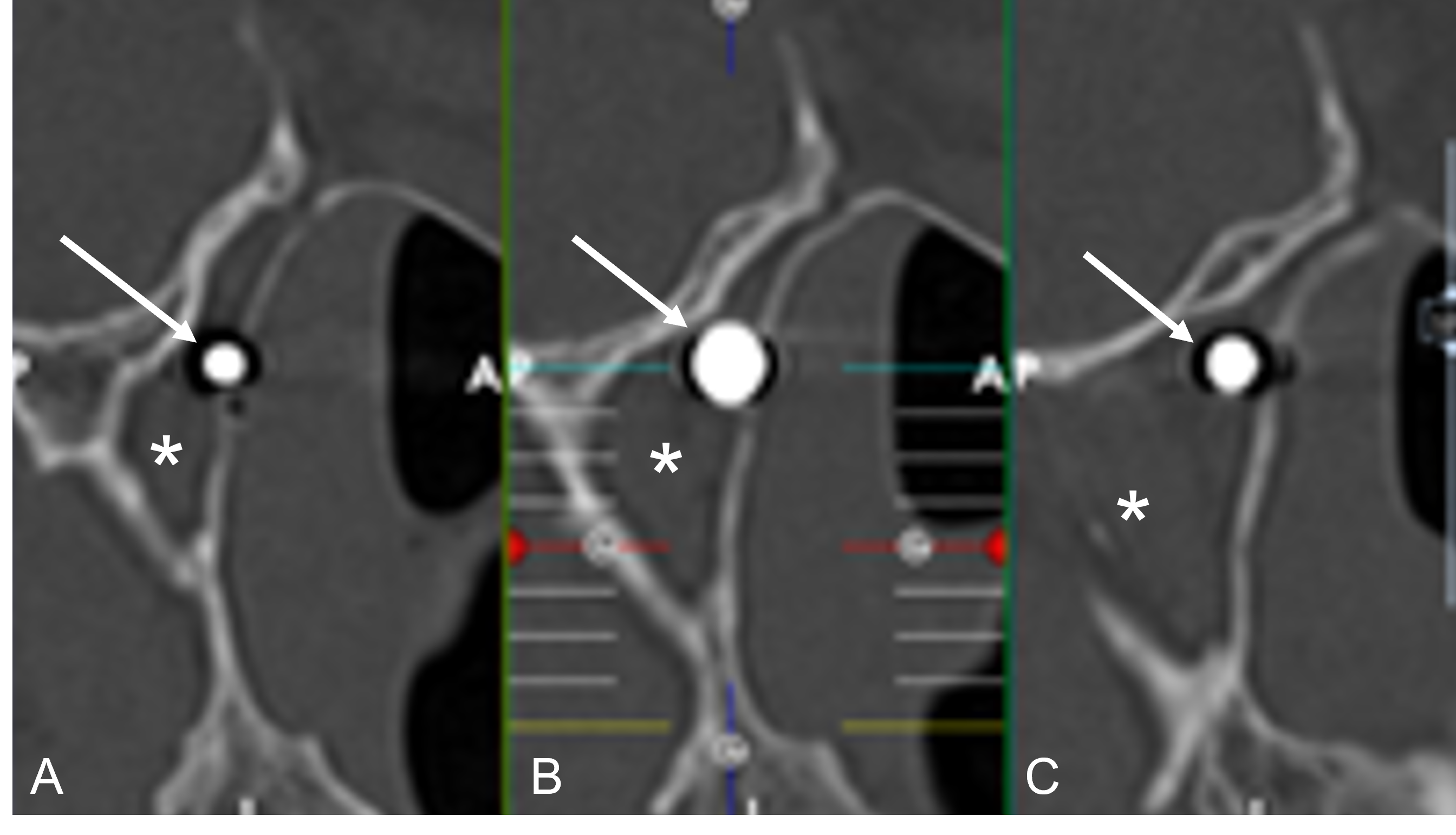
Pallister-Killian Syndrome (PKS) is a rare genetic disorder characterized by the mosaic presence of a supernumerary isochromosome consisting of two short arms of chromosome 12, leading to a variety of complications, including those related to oral and dental health. This case report marks the first case report on the dental characteristics of a patient with PKS using cone beam computed tomography (CBCT). A 17-year-old female with PKS was reported exhibiting bilateral maxillary sinus hypoplasia, along with taurodontism in teeth n°15 and n°16, and an unusual “crayon-like” morphology in teeth n°14, n°15 and n°25. Moreover, hypoplasia of the sphenoidal sinuses, accompanied by left sphenoidal sinusitis, was noted.
A multidisciplinary dental approach is advocated for managing individuals with PKS. Further research incorporating a larger sample is critical to comprehensively assessing the dental features of PKS using dental radiography. Additionally, the development of an open-source CBCT database cataloging dental characteristics for rare dental conditions, including PKS, may be a suitable tool to access to reference images and to share information on orphan diseases with dental implications.
Les salmonelles sont des bactéries d’origine alimentaire pouvant occasionner des gastro-entérites, des bactériémies et des infections locales par dissémination hématogène. Nous présentons le cas d’un jeune patient d’origine malienne ayant développé un abcès lingual à Salmonella typhi. Cette présentation, rare, n’a pas encore été décrite dans la littérature scientifique. Le diagnostic a été posé par analyse bactériologique suite à l’incision et au drainage de l’abcès. Une antibiothérapie à large spectre a été instaurée et adaptée en fonction des résultats de la culture. Cet article rapporte le premier cas documenté d’abcès lingual causé par Salmonella typhi.
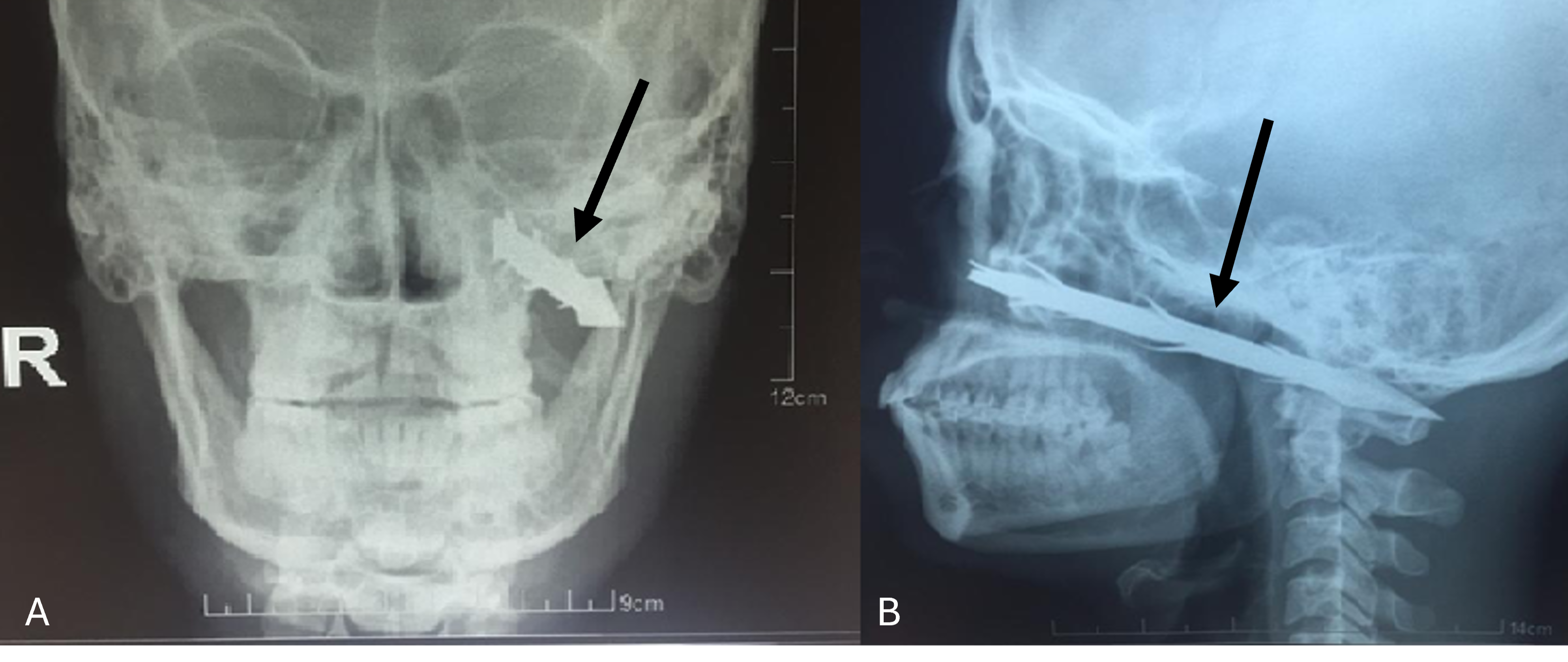
An arrow maxillofacial penetrating injury is an unusual traumatic injury sometimes encountered in developing countries. This rare injury has the potential to be dangerous because the arrow is deeply lodged in maxillofacial region crossed by major vessels, and because damage to one of these vessels should always be suspected. Furthermore, removal of a foreign body may result in complications such as massive bleeding or iatrogenic injury to adjacent structure and complications should always be considered in maxillofacial region. We describe a case of a patient who presented with maxillofacial penetrating arrow injury and analyze the problems faced in its management with emphasis on diagnostic imaging, on surgical planning and on careful surgery management.
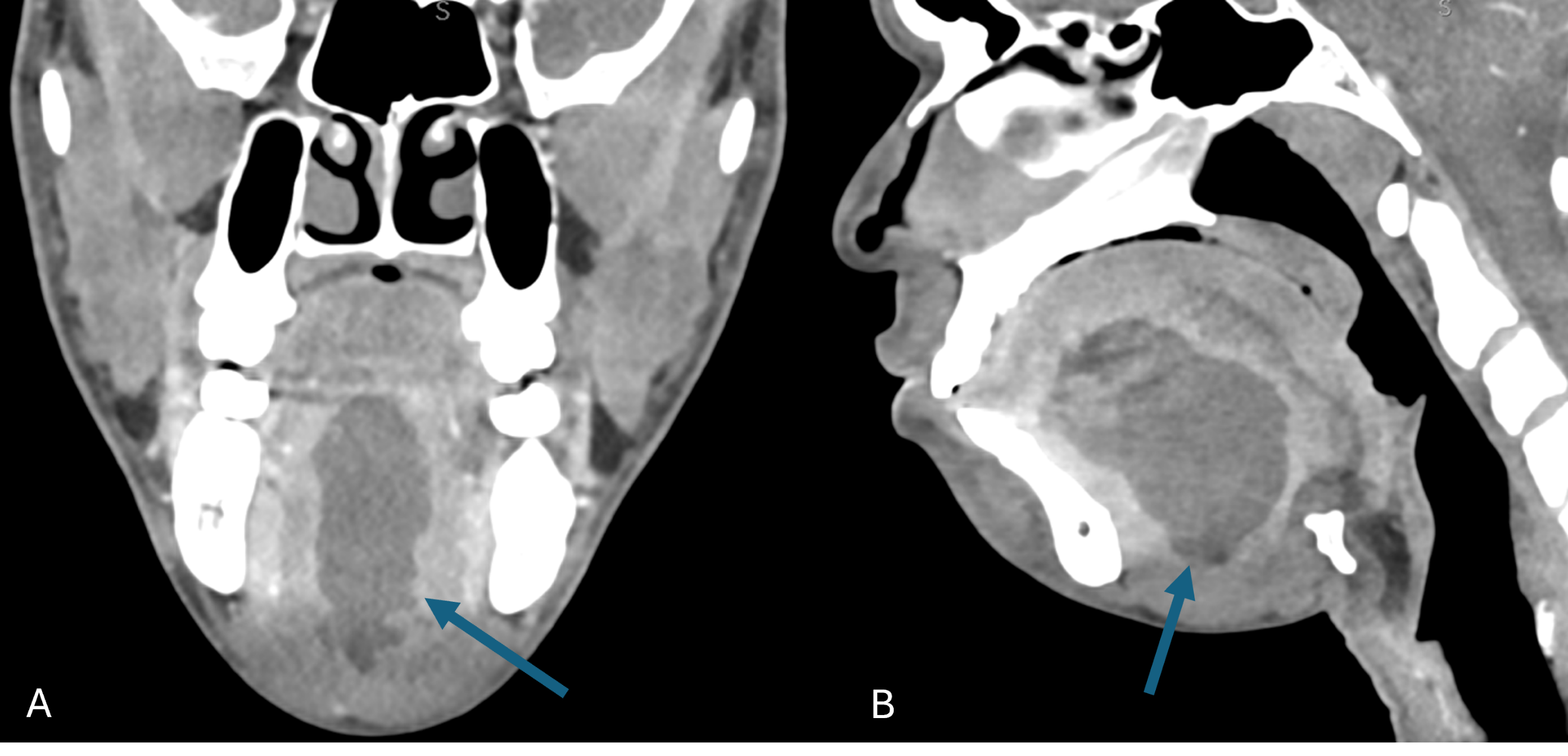
Cutaneous metastases occur in 0.5 to 9% of all cancers. Esophageal cancer is one of the most aggressive cancers worldwide. Most cutaneous metastases from esophageal cancer were related to squamous cell carcinomas. Few cases have been described about cutaneous metastases related to esophageal adenocarcinomas. These metastases mostly affect patients over 60 years-old, and present as cutaneous asymptomatic nodules.
A 69-year-old male presented with a painless and extensive left neck cutaneous induration and erythema. The lesion that was initially diagnosed as a dental cervical cellulitis by his dental practitioner. The patient was known since 2019 to suffer from a esophageal adenocarcinoma whose first treatment was surgery. The patient was currently under immunotherapy for a local recurrence. We firstly assessed the uncommon cervical cellulitis by carrying out an injected head and neck computed tomography (CT) scan which showed an unspecific skin, dermal and muscular infiltration of the left cervical region. The 18-FDG PET/CT demonstrated a suspicious fixation of the neck that was followed by a skin biopsy. The histological and immunohistochemical examination showed the metastatic adenocarcinomatous origin of the cervical skin lesion. The patient was upstaged to a stage IV of his esophageal cancer and started palliative chemotherapy.
Special attention must be paid in case of diffuse cervical skin infiltrations, even in the presence of a dental infection, in patients with cancer, in order to perform the correct diagnosis.
The solitary median maxillary central incisor syndrome (SMMCI) is a rare autosomal dominant genetic syndrome characterized by the presence of a single central incisor positioned along the midline in both primary and permanent dentition. It is often associated with the holoprosencephaly spectrum, a group of brain and facial malformations. The etiopathogenesis of SMMCI is believed to involve embryonic developmental defects occurring between the 35th and 38th day of gestation, primarily affecting midline facial structures. Several genetic factors, including mutations in the Sonic Hedgehog gene on chromosome 7 and other genetic variants, have been implicated in SMMCI development. Diagnosis is typically made through clinical examination, prenatal ultrasound, and postnatal dental evaluation. Management of SMMCI requires a multidisciplinary approach involving pediatricians, otolaryngologists, neuro-pediatricians, and genetic counselors. Dental interventions may include extraction and space maintenance, orthodontic treatment, prosthodontic options, or esthetic considerations. Further research is needed to understand better the underlying mechanisms and genetic factors associated with SMCI, which will contribute to improved diagnosis and management of this syndrome.
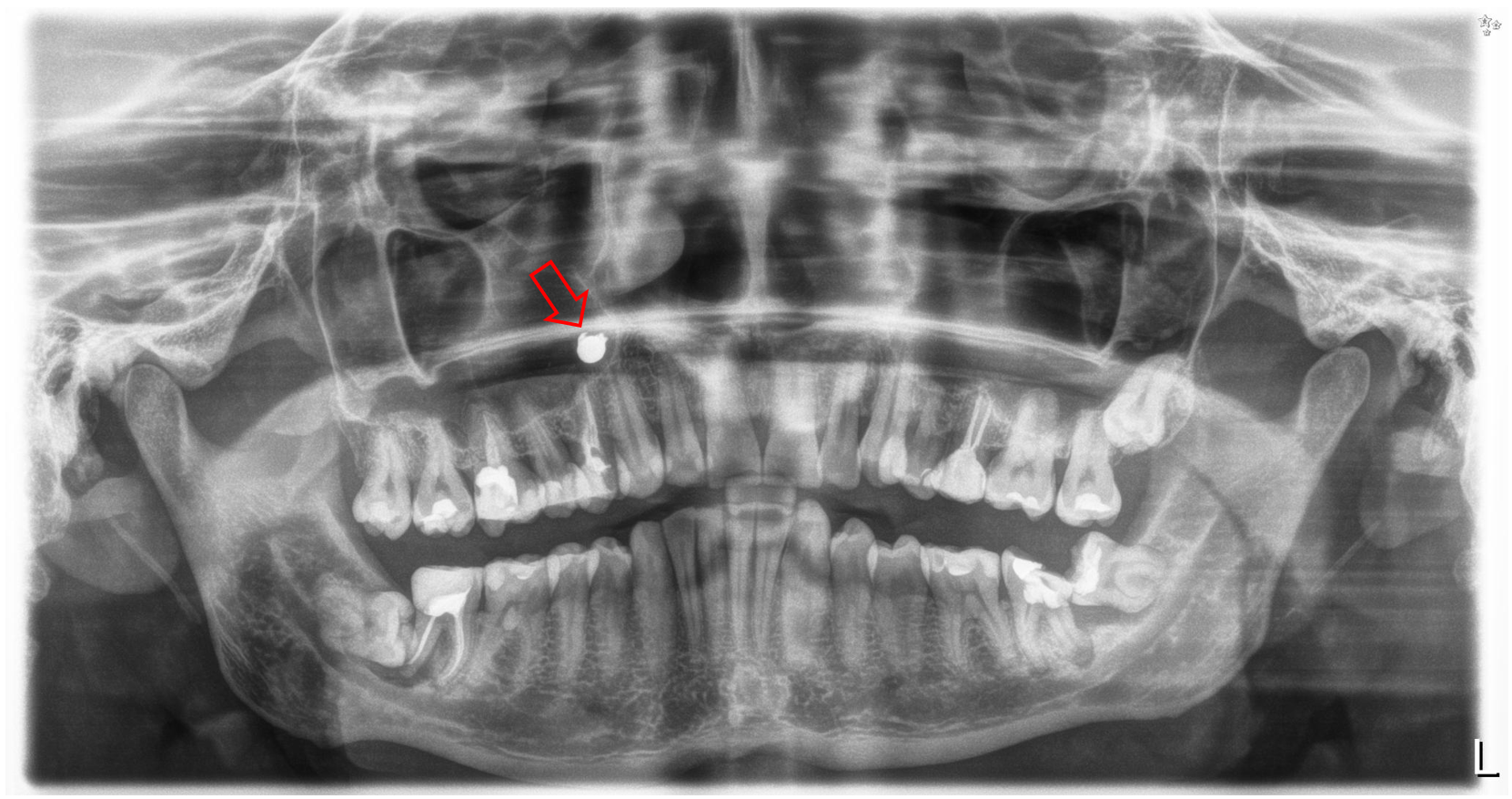
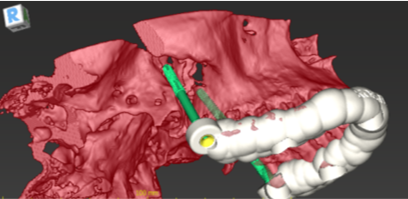
Gunshots with non-powder weapons are relatively common in children, and most of them occur unintentionally. This paper describes the second known case of an adult male in whom a shot from an airgun resulted in the presence of a projectile within the maxillary sinus. A 47-year-old man was shot inadvertently about 10 years earlier and was asymptomatic at the time of reporting. The presence of a foreign body detected on a routine orthopantomogram was confirmed by a medical interview and a three-dimensional radiological examination. The pellet located in the right maxillary sinus was removed from intraoral access through the anterior wall of the sinus. The course of the surgical procedure was complicated by the projectile dislocation in relation to the position determined by radiological examinations. Postoperative care and a 4-year follow-up period were uneventful. The maxillary sinus may be considered a favorable location for a persistent projectile, which may reside in the maxillofacial region asymptomatically for many years. The foreign body may move loosely in the maxillary sinus, which should be taken into account when planning an operation.
Objective: Taurodontism is a developmental disorder with enlargement of the body of the tooth and lack of cervical constriction, which results in a large pulp chamber and small roots with the apical displacement of furcation. Taurodontism exists in deciduous, and definitive unilateral, and bilateral teeth. We found that taurodontism was also described in 67 syndromes. We proposed a review of the open access literature on taurodontism, a new clinical classification of taurodontic teeth with illustrations from free open access literature, and from our case serie of 15 patients.
Material and methods: We performed a systematic search for articles with free full text about taurodontism. The search was performed by one observer in PubMed database. We found 168 articles, and after application of inclusion/exclusion criteria we finally selected 136 articles for the review.
Results: we provided 34 figures of taurodontic teeth related to: 1) Unilateral mandibular first premolar, 2) Unilateral mandibular second premolar, 3) Bilateral mandibular first and second premolar, 4) Bilateral upper maxillary first premolars, 5) Bilateral mandibular second molars, 6) Bilateral upper maxillary second premolar and left first molar, 7) Bilateral upper maxillary third molars, 8) Bilateral upper maxillary first and second molars, 9) Bilateral upper maxillary first, second, and third molars, 10) Bilateral upper maxillary molars (third molars, second, and first left upper molars), and mandibular molars (first right, and left mandibular molars, right third molar), 11) Bilateral upper maxillary molars (first, second, third right, and left upper molars), and mandibular molars, 12) Unilateral first mandibular premolar with cleft, 13) Bilateral molars of the mandible and the upper maxilla (adolescent patient who received chemotherapy at the age of 3-years-old to treat retinoblastoma), 14) Unilateral first maxillary molar (Treacher-Collins syndrome).
Conclusions: We proposed a new clinical classification of taurodontic teeth based on hypo-, meso-, and hypertaurodontism, and on different types of deciduous, and definitive teeth (42 boxes). We were first to provide free reference images for: 1) upper maxillary second premolar hypertaurodontism, 2) mandibular second premolar mesotaurodontism, 3) upper maxillary third molar meso-and hypertaurodontism, 4) mandibular first molar hypotaurodontism, 5) mandibular third molar mesotaurodontism. We were also first to freely illustrate taurodontism related with chemotherapy, cleft palate patients, and Treacher-Collins syndrome.

Le syndrome de Langenbeck ou hyperplasie des processus coronoïdes mandibulaires est une maladie rare caractérisée par une augmentation de volume des processus coronoïdes. Cette hyperplasie entraîne un conflit osseux limitant l’ouverture buccale. Ce syndrome doit être connu des cliniciens car il entre dans le diagnostic différentiel des limitations d’ouverture buccale. Nous présentons un cas traité avec succès dans notre service. Une prise en charge efficace comporte un versant chirurgical et kinésithérapeutique, qui sont discutés dans notre publication.
Objective: Sphenopalatine ganglion block remains a noninvasive therapeutic option to treat diverse facial pain syndromes. The aim of this case report was to verify the effectiveness and safety of three-dimensional (3D) injection guide for sphenopalatine ganglion block in a tongue cancer patient.
Case report: A 53-year-old man presented with a large squamous cell carcinoma of the right base of the tongue, classified cT4N2M0 and exhibiting excruciating facial pain. A botulinum toxin injection was performed following Dr. Yoshida’s method, using a 3D injection guide.
Conclusions: Sphenopalatine ganglion block with 3D injection guide can be an effective treatment against cancer pain. In this case report a complete withdrawal of painkillers was obtained less than 24 hours after botulinum toxin injection.
Objective: to present and to illustrate a new methodology for daily practice in cone beam computed tomography (CBCT) interpretation and reporting in cleft lip palate (CLP) non syndromic paediatric patients. The proposed protocol is based on clinical experience and on systematic search of the literature.
Material and methods: We performed two types of systematic search of articles: 1) articles related to the use of CBCT in CLP patients, and 2) articles related to the reporting and interpretation of the CBCT images by radiologists. We used two databases PubMed and Google scholar.
Results: For indications of CBCT in CLP patients we found in PubMed 378 articles and 48 articles were selected for the review; in Google scholar we found 463 articles, and 9 articles were selected for the review. 2) For reporting in CBCT we found 956 articles in PubMed, and 9 articles were selected for the review.
Conclusions: We presented the 6-steps system for interpretation and reporting information from CBCT of CLP paediatric patients: 1) Step 1 (axial view): presence or absence of bone bridge remnants of alveolar bone graft; Step 2 (3D dental tissue reconstruction): description of dental arch tooth, search for agenesis and supernumerary teeth, description of variation in the position of the tooth explaining the type of existing translation and rotation; Step 3 (coronal view): cleft palate pathway and its extension; anomaly in maxillary, ethmoid and sphenoid sinuses if existing; Step 4 (sagittal and coronal view): checking of the opening (calcification sites) of the sphenooccipital synchondrosis, and checking of anomalies of the occipital bone; Step 5 (3D bone tissue reconstruction): C1-C2 vertebra anomalies; Step 6 (3D soft tissue reconstruction): external ear anomalies. We illustrated our methodology with 46 figures from 5 CBCT of CLP patients.
Objective: To present a pictorial review on central mucoepidermoid carcinoma.
Case report: Central mucoepidermoid carcinoma (CMEC), also known as intraosseous mucoepidermoid carcinoma (IMEC), is an extremely rare disease (less than 2-4% of all MEC). However, CMEC is the most frequent malignant salivary gland tumour found in intraosseous locations. Due to this unusual location, diagnosis of CMEC can be challenging. Therefore, CMEC is often mistaken for other intraosseous or odontogenic pathologies. Radiological assessment should include panoramic X-Ray, CBCT and thoracic CT, which should be performed after diagnosis. The recommended treatment includes radical resection surgery, followed by radiotherapy if indicated. A long-term follow-up is recommended for up to 10 years.
Conclusion: The authors experienced the challenging diagnosis of CMEC through the case of a patient who presented with a slowly growing palatal mass.

Objective: Paracondylar (PCP) and epitransverse processes (ETP) represent rare types of articulations that can occur between the occipital bone and the transverse process of atlas vertebra.
Material and methods: Five systematic search strings were conducted on PubMed database on 14.01.2022. The search was conducted by one observer to identify studies on PCP, and on ETP in living patients. Open and close access articles were selected as this topic is infrequently described in the main medical literature.
Results: We provided with a pictorial review of 1) Paracondylar tubercle, 2) Unilateral PCP with cylindrical shape, 3) Unilateral PCP with pyramidal shape, 4) Unilateral PCP with lateral joint with transverse process, 5) Unilateral PCP with superior joint and partial fusion with transverse process, 6) Unilateral ETP with neo-condyle and joint with occipital condyle, 7) Unilateral ETP with joint with occipital bone, 8) Unilateral ETP with a bony bridge with lateral mass (ponticulus lateralis), and 9) Bilateral variation: paracondylar mass and ETP.
Conclusions: Six figures were found in the selected literature and belong only to articles published in closed access. We provided with additional 41 open access freely available figures. We were first to present CBCT reference figures of: 1) Unilateral paracondylar tubercle, 2) Fusion of PCP with the transverse process of C1, 3) Joint between ETP and the lateral side of occipital condyle, and 4) Presence of bony bridge (ponticulus lateralis) between ETP and the lateral mass of C1. We were also first to describe a bilateral mixt variation with paracondylar mass on one side and ETP on the other side of C1. An open and accessible knowledge support (such as Nemesis journal) is needed to easily find clinical reference CBCT figures of craniocervicofacial bone variations.
Objective: First cases of osteonecrosis of the jaw in patient exposed to bisphosphonates were presented in 2003. Bisphosphonates related osteonecrosis of the jaw (BRONJ) was further extended to medication-related osteonecrosis of the jaw (MRONJ) to include antiresorptive and anti-angiogenic drugs. Some directives were described for the treatment of this disease in function of its gravity. Treatments of high stage of MRONJ are subject to discussion because of their morbidity. Complete healing is difficult to reach and often needs combination of invasive and non-invasive treatment.
Case report: We report and illustrate a clinical case of new bone formation after MRONJ on pamidronate and zoledronate treatment for multiple myeloma. The treatment of choice was sequestrectomy and conservative treatment.
Discussion: The consensus to reach a complete healing after MRONJ is not already known. More studies are needed.
Objectif: Déterminer quels étaient les sujets et le contenu des publications réalisées par des chirurgiens oro-et maxillo-faciaux pratiquant quotidiennement dans les pays à moindre ressources d’Afrique sub-saharienne (ASS).
Matériel et méthodes: Nous avons utilisé deux bases de données, PubMed et African online journals, pour cette revue de littérature. Nous avons limité notre recherche aux années 2000-2022. Nous avons choisi les articles avec le résumé et uniquement en langue anglaise ou française. Pour chaque article nous avons cherché le pays d’origine, la langue de l’article, l’accessibilité des articles ; le nom du journal, le nombre et le type d’illustrations. Pour chaque article en accès libre, nous avons cherché le mode de payement de la publication et la cession les droits d’auteur. Nous avons trouvé 1761 articles et retenu finalement 47 articles.
Résultats: Les publications issues des pays ASS sont très rares parmi toutes les publications du continent africain (47/1761= 2,6%). Tous les articles retenus étaient publiés dans 33 journaux différents. 46,8% des articles ont été écrits par les auteurs de Tanzanie et de Soudan. Les articles en accès libre représentent la majorité des articles publiés (59%). Les articles en accès fermé sont liés au Noma et aux articles en langue française. Nous avons identifié uniquement deux journaux scientifiques African Health Sciences et South Sudan Medical Journal, qui étaient gratuits pour les lecteurs et les auteurs. La langue anglaise était prédominante (85%). 53 images étaient accessibles gratuitement pour illustrer l’ensemble des sujets de la chirurgie orale et maxillo-faciale dans les pays ASS. Nous avons également présenté les conclusions des articles en les classant par sujets : 1) Tumeurs (13 articles), 2) Traumatismes/fractures maxillo-faciales (11 articles), 3) Fentes (4 articles), 4) Pathologies infectieuses (5 articles), 5) Pratiques culturelles (4 articles), 6) Noma (2 articles), 7) Syndromes (5 articles), et les sujets divers (3 articles).
Conclusions: Nous avons présenté le système de publications scientifiques actuelles, la place des publications scientifiques et les aspects particuliers des publications sur la chirurgie maxillofaciale dans les pays ASS, nous avons proposé de possibles directions de publication pour les auteurs chirurgiens maxillo-faciaux des pays ASS, ainsi que la place potentielle de la revue Nemesis dans ce contexte africain.
Objective: The aims of this systematic review of the literature were to investigate the uses of cone beam computed tomography (CBCT) in pediatric dentistry and, if possible, identify the indications.
Material and methods: A literature search was conducted using the PubMed and Scopus electronic databases and the keywords "CBCT and pediatric dentistry". This search provided us with 1518 references. The selected publications were all clinical articles written in French or English and referring to a pediatric population. After screening, 461 eligible full text articles remained.
Results: In total, there were 169 references that met the inclusion criteria. Different topics, mainly relating to orthodontics, anatomy, and cleft lips and palate, were discussed. There was large variability in the information concerning the technical parameters. The radiographic protocols that we analyzed showed a large heterogeneity.
Conclusions: The level of evidence provided by our work is limited because only two randomized double-blind controlled studies are included. Two indications can be distinguished: for orthodontics and for the rehabilitation of cleft lips and palate. There are a multitude of radiographic protocols. More research is needed to identify other potential clinical indications as well as to determine a standard CBCT protocol for children and adolescents.
Objective: This article focuses on the penetrating trauma of the facial mass caused by the knife with retention of the blade fractured in the facial skeleton.
Case report: We describe preoperative, intra-operative and post-operative outcomes of the knife stabbing in the face, and of the surgical removal of the broken 8cm long blade using two dimensional, and tridimensional computed tomography, and clinical iconography
Conclusions: We provide the readership with a broader perspective on iatrogenic facial trauma caused by blades with examples from history of medicine, with biomechanical focus, as well as a review of literature on the management, and on the surgical treatment outcomes of such infrequent emergency in maxillofacial surgery.
Objective: Firstly, this review aims to analyse the recent literature about three-dimensional (3D) diagnostic imaging in complex and compound odontomas and compare it to two-dimensional (2D) imaging. Panoramic radiographs help to evaluate the vertical position of odontomas, and occlusal radiographs are used to evaluate the proximity to adjacent teeth. However, cone beam computed tomography (CBCT) can offer volumetric images, and therefore, a more accurate three-dimensional analysis. Secondly, this research aims to construct an open classification matrix for complex and compound odontomas for dentomaxillofacial CBCT radiology protocols based on a systematic literature review.
Material and methods: Two systematic literature searches were conducted in PubMed (Medline), on 2 February 2022 concerning classification systems, and on 5 February 2022 concerning CBCT images.
Results: In total, these searches revealed 391 papers by reviewing the databases mentioned above. Six articles were selected for inclusion on classification of odontomas and 13 articles were found on CBCT imaging. Consequently, the construction of an open classification matrix for compound and complex odontomas for dentomaxillofacial CBCT radiology protocols was performed using these 19 articles.
Conclusions: CBCT offers a more precise position and accurate diagnosis of complex and compound odontomas compared to 2D imaging. Consequently, it enhances the detailed view of the site (multiple or unique), location (intraosseous, partially or completely extragnathic), size, extension (bony expansion, thinning or perforation cortical bone), density and type (denticulo type, particle type, denticulo-particle type, denticulo-amorphous type, amorphous tissue), relationship (with the crown or root of the definitive tooth), adjacent teeth resorption (deciduous or definitive), adjacent teeth (retention or impaction), and distance with adjacent structures (inferior alveolar nerve, sinus maxillaris), as well as adequate surgical planning. Moreover, this research presents an open classification matrix for the most complete description of compound and complex odontomas when analysing CBCT imaging.
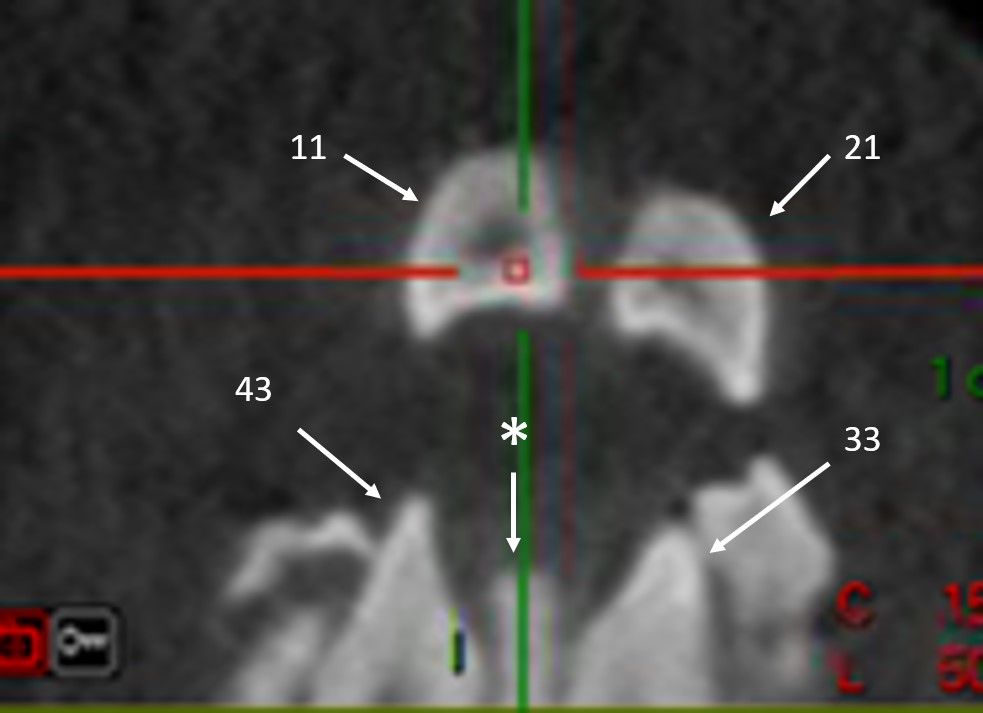
Objective: To describe dentoalveolar findings in one pediatric patient with a very rare Carpenter syndrome or acrocephalopolysyndactyly type II, and using cone beam computed tomography (CBCT).
Case report: We found a syndromic oligodontia, upper canine transmigration, and an exceptional agenesis of four lateral incisors. We also described the fourth case in the literature of a single solitary lower incisor on the midline, and the first case ever illustrated on CBCT.
Conclusions: We proposed and illustrated the use of the system of progressive numbering of teeth on CBCT axial views to better understand complex dental clinical situations such as syndromic oligodontia.
